Natural disasters have severe and often traumatic implications for affected individuals and their communities. Evidence suggests that preventative mental health interventions, primarily designed to improve resilience and wellbeing, can provide individuals and communities with resources to ‘bounce back’ from adversity and decrease the risk of future psychological distress or mental illness.
Experience of disasters can lead to a higher risk of developing mental illness such as depression, and more immediately, decreased levels of wellbeing and flourishing.1 These two constructs, mental illness and wellbeing, are often thought of as polar opposites. However, they are related but separate constructs, with both playing an important and dynamic role in the mental health of individuals.2 This distinction is an important one, as both wellbeing and mental illness should be considered separate targets for intervention prior to, or following a disaster situation.
Although a period of gradual recovery from mental illness symptoms is witnessed for a large proportion of people affected by natural disasters, many suffer throughout the process.3 After a disaster, mental health service providers may have greater difficulty engaging with people because they may not display clinical mental illness symptoms or do not wish to talk with a counsellor or psychologist, or they live in regional or rural communities with problematic access and attitudes to mental health services.4
Teaching basic psychological skills to improve positive mental health outcomes, such as wellbeing and resilience, can mitigate the immediate effects of the disaster on the individual. It can improve and maintain positive mental health outcomes that help individuals to ‘bounce back’ quicker and decreases the risk of developing psychological distress down the track.5 Similarly, using positive mental health interventions to upskill people and communities before the disaster actually occurs (i.e. using a primary prevention strategy), may play an important and protective role in the mental health of individuals regardless of whether disaster strikes or not.6 Interventions targeting individual community members may be a cost and time effective solution that can be offered in conjunction with other services. An example woud be interventions delivered at the interpersonal, community or societal level7 aimed at restoring the communities after a disaster (see Figure 1 for an explanatory model).
Wellbeing training
A pilot project to deliver a resilience training program to a rural community affected by a significant bushfire was conducted by the South Australia Health and Medical Research Institute Wellbeing and Resilience Centre and the South Australia Department of Human Services. The training was offered in the rural community affected by the Pinery fire that caused catastrophic losses in several communities in South Australia’s lower midnorth in 2015. The bushfire burnt 86,000 hectares of land, destroyed 97 homes, caused extensive damage to property and losses of livestock and crops with an estimated $88 million in insured losses. Tragically, two people died in the fires.
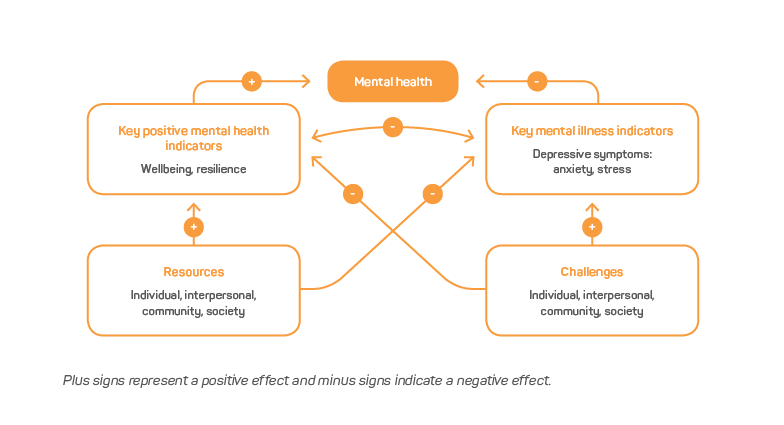
Figure 1: A conceptual model of the interplay between positive mental health outcomes and outcomes associated with mental illness. Plus signs represent a positive effect and minus signs indicate a negative effect.
The pilot program offered members of the community a suite of practical skills to build their personal resilience that would be useful. The training included ten ‘resilience skills’. These originated from best-practice positive psychology interventions such as mindfulness, as well as techniques stemming from well-accepted psychological therapies such as Cognitive Behavioural Therapy.8 The skills included adaptability, positive coping, self-regulation and social support to improve wellbeing and resilience. In particular, the training focused on knowledge creation, skills building and improvement of behavioural capacity.
The training was delivered using a train-the-trainer model where the trainers teach a selected group of community members to deliver the skills training to residents living in the fire-affected communities. The goal is to embed aspects of wellbeing and resilience into community ethos.
To evaluate the pilot program, consenting participants provided data used to measure their wellbeing, resilience and psychological distress before and after the training, as well as training satisfaction questions. Encouraging results were achieved despite the small sample size (n=28 at time 1, n=13 at time 2). Participants who completed both surveys indicated significantly higher levels of resilience (p=.03, Cohen’s d=0.2). Additionally, non-significant increases were found for wellbeing and psychological distress when comparing before and after scores (Cohen’s ds of 0.31 and 0.56, respectively).
Qualitative feedback on the training was also positive. Participants reported a high degree of confidence in the quality of the trained community trainers and reported that the content was understandable, useful and engaging. All participants either strongly agreed or agreed that people would benefit from the resilience skills and equally felt that the training prepared them to use the skills learnt. There was a strong sentiment that the skills would be useful across the entire community and participants indicated they would be very likely to recommend the training to others. This feedback was represented by a quote from one participating community member:
I have begun to use skills and will continue to have a more effective life for myself and those around me. Thanks to all of you for supporting our community following the fires.
These results should be interpreted with caution due to limitations of study design, the small sample size and challenges associated with a real-word implementation of a program (e.g. attrition during intervention) in a disaster-affected community. However, its positive reception and indications of positive effects on relevant mental health outcomes provide an encouraging basis for future exploratory work.
Future work should focus on ‘future proofing’ communities that are prone to natural disasters by upskilling local trainers and involving communities and local partner organisations to consider the wellbeing and resilience of individuals and communities before critical events occur. Importantly, training should be offered in conjunction with established mental health services (we do not recommend this training is a replacement for clinical intervention). The goal is to build psychological health at the individual and community level. Improving the resilience of individuals contributes positively to community social capital that, in turn, builds community resilience.
Footnotes
- Fergusson DM, Horwood LJ, Boden JM & Mulder RT 2014, Impact of a major disaster on the mental health of a well-studied cohort. JAMA psychiatry, vol. 71, pp. 1025-1031.
- Keyes CLM 2005, Mental illness and/or mental health? Investigating axioms of the complete state model of health. Journal of consulting and clinical psychology, vol. 73, p. 539.
- Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E & Kaniasty K 2002. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry: Interpersonal and biological processes, vol. 65, pp. 207-239.
- North CS & Pfefferbaum B 2013, Mental health response to community disasters: a systematic review. JAMA, 310, pp. 507-518.
- Bolier L, Haverman M, Westerhof GJ, Riper H, Smit F & Bohlmeijer E 2013, Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health, vol. 13, p. 119.
- Howlett JR & Stein MB 2016, Prevention of trauma and stressor-related disorders: a review. Neuropsychopharmacology, vol. 41, p. 357.
- Norris FH, Friedman MJ & Watson PJ 2002, 60,000 disaster victims speak: Part II. Summary and implications of the disaster mental health research. Psychiatry: Interpersonal and biological processes, vol. 65, pp. 240-260.
- Leppin AL, Bora PR, Tilburt JC, Gionfriddo MR, Zeballos-Palacios C, Dulohery MM, Sood A, Erwin PJ, Brito JP & Boehmer KR 2014, The efficacy of resiliency training programs: a systematic review and metaanalysis of randomized trials. PloS one, October 2014. doi.org/10.1371/journal.pone.0111420.